There are few policy areas more weighted with urgency, emotion, and concern than childhood obesity. For more than two decades, governments across the world have wrestled with rising rates of childhood obesity, often gravitating towards interventions that feel immediate, visible, and controllable. Advertising restrictions of “less healthy food” (LHF) have become one of the most politically attractive tools to address the issue. Their appeal is obvious. Restrictions can be implemented with minimal direct cost to taxpayers and deliver an immediate sense of action. They allow policymakers to signal concern without confronting the deeper socioeconomic roots of childhood obesity.
Yet such policies are largely based on assumption and association rather than evidence. The belief that advertising meaningfully contributes to childhood obesity rests more on intuition than science. It is a belief nurtured by the high visibility of advertising, the overestimation of its persuasive power, and a misunderstanding of the role it plays in mature markets such as those in the UK. The question — does advertising cause childhood obesity? — is rarely examined with sufficient rigour in public debate. When it is, a striking pattern emerges: advertising is not a causal driver of childhood obesity, and further restrictions are unlikely to produce meaningful improvements in children’s health.
This essay summarises the findings of a comprehensive review of the existing scientific literature to identify the best currently available knowledge on1:
- the primary causes of childhood obesity;
- whether advertising is a significant causal factor associated with childhood obesity;
- whether advertising of less healthy foods drives increased consumption;
- whether advertising restrictions and bans are likely to be effective in reducing consumption of less healthy food; and
- what types of initiatives/programs, if any, have been found to show promise for reducing the prevalence of children being overweight.
To understand why, policymakers must resist the seductive simplicity of advertising-as-cause and instead engage with what the empirical research shows. And in doing so, a very different picture emerges, one in which childhood obesity is shaped overwhelmingly by early-life biological, socioeconomic, and behavioural factors, while advertising plays, at most, a limited and short-lived role in shaping food choice. And most importantly, that limited role does not translate into weight gain.
What follows is an argument grounded in the strongest available evidence, a narrative that reframes the policy discussion not out of deference to industry, but out of respect for scientific truth. If we want to reduce childhood obesity, we must stop regulating factors that do not impact the problem and start investing in the ones that do.
The incorrect belief that advertising drives obesity
The assumption that advertising is a major contributor to childhood obesity has an intuitive pull. Advertising’s purpose is to persuade; therefore, the more advertising children see for unhealthy foods, the more unhealthy foods they will want to eat. If they eat more unhealthy foods, they will gain more weight. And if they gain more weight, higher obesity rates will follow.
This linear storyline has dominated public debate, but crucially it is not supported by the available evidence. A large body of cited studies across medical, health, and business research, including multiple meta-analyses, have examined the causal factors associated with childhood obesity. Not surprisingly, most such studies originate from the medical community and appear in medical journals. They have found that maternal pre-pregnancy weight, high birth weight, rapid weight gain in the first year of life, breastfeeding duration, sleep patterns, and socioeconomic conditions shape children’s weight trajectories well before commercial messaging is a factor in their life.
This is a consistent conclusion across literally hundreds of studies. Large-scale reviews and meta-analyses, such as those by Weng et al. (2012), Poorolajal et al. (2020), and the massive 419-study analysis in China by Jiang et al. (2025), identify numerous early-life and behavioural risk factors. None identify exposure to LHF advertising as a significant cause. In the majority of cases, advertising is not even measured because researchers do not consider it sufficiently plausible to include among candidate predictors. To reduce childhood obesity, policymakers must focus on the following risk factors that consistently emerge as significant in the research literature:
- Early-life factors – maternal obesity, gestational weight gain, high birth weight, rapid infant weight gain, early feeding patterns, and breastfeeding duration play powerful roles in shaping long-term BMI. Interventions at this stage have the greatest potential for impact.
- Socioeconomic determinants – childhood obesity is strongly socially patterned. Lower-income households face food insecurity, reduced access to safe play spaces, higher exposure to stress, and fewer opportunities for structured physical activity. These factors cannot be offset by regulating commercial messages.
- Dietary patterns shaped by environment – sugar-sweetened beverages, large portion sizes, and frequent snacking are consistently associated with higher obesity risk. These behaviours reflect habits, routines, price structures, and availability, not advertising exposure.
- Sleep, physical activity, and screen time – insufficient sleep and low physical activity are reliable predictors of obesity. These are lifestyle and environmental issues, not advertising issues.
- Family and school environments – regular family meals, active routines, school-based physical activity programmes, and high-quality school meals show positive effects on children’s weight.
None of these drivers are meaningfully addressed by LHF advertising restrictions. Meanwhile, in the policymaking imagination, advertising looms large precisely because it is visible. It is easier to point to a billboard, a television spot, or a digital animation than it is to tackle maternal stress, housing conditions, shift work, or chronic socioeconomic disadvantage. Advertising can be easily restricted by regulation; inequality cannot. Thus, advertising regulation becomes the solution – culturally convenient, politically manageable, and symbolically satisfying. But symbolic policies rarely solve structural problems.
Short-term preferences do not equal long-term weight gain
Whilst it is true that multiple studies find that exposure to LHF advertising affects children’s immediate preferences for unhealthy food, short-term consumption, and purchase intention, the weight of the evidence shows weak or no correlation between food advertising and the “bottom line” measures of higher body mass index (BMI) or childhood obesity rates. Indeed, studies that control confounding factors such as screen time, socio-economic status, mother’s or father’s weight, and dietary factors show no significant association between LHF advertising and BMI or childhood obesity rates.
In addition, the associations found between LHF advertising and consumption/preference measures can also be questioned due to measurement issues, including problematic measures of advertising exposure, self-reported obesity data, and a lack of longitudinal data on BMI. Experiments do show that children exposed to ads featuring crisps or sweets will temporarily prefer those items or consume slightly more when snacks are presented immediately afterwards. These findings are often cited as proof that advertising contributes to obesity. But such an interpretation requires a leap that the studies themselves do not support. Short-term behavioural nudges under controlled conditions do not equate to sustained increases in daily caloric intake, and these studies do not reflect how ASA-regulated advertising exists or operates in the real world.
Table 1 summarises the measurement and methodological issues that have been common in studies of the impact of LHF advertising exposure on childhood obesity.
Table 1: Methodological and Measurement Issues in Studies Relating Exposure of Advertising for Less Healthy Foods to Childhood Obesity
| Problem Area | Explanation | Why It Is Important |
| 1. Inappropriate extrapolation to other dependent variables |
While some studies find effects on preference, purchase intent, or short-term consumption, these are not measures of long-term impact on weight |
The weight of the evidence of the literature on exposure to LHF advertising does not support a long-term effect on children being overweight or obese |
| 2. Measures of Advertising Exposure | Many studies use self-reported measures of advertising exposure. | Self-reported advertising exposure measures are problematic; relies on recall of a subset of viewing and is especially difficult for children |
| 3. Use of Advertising Spending as Proxy for Exposure |
Studies assume that advertising spending levels in an area capture an individual’s exposure to ads.
|
Advertising spending is a poor proxy for actual exposure to ads, especially for children. Even more true in recent years as media fragmentation has accelerated. |
| 4. Confounding Factors | Screen time correlates with sedentary behavior, diet, socio-economic status, parenting → hard to isolate ad effects. | Several studies that take into account confounding factors such as screen time, sedentary behavior, availability of healthy foods, socioeconomic status, etc., find no correlation between LHF advertising and childhood obesity |
| 5. Reverse Causality | Some children with higher BMI may consume more media, leading to more advertising exposure. | Children with higher BMI may consume more media and see more ads as a result of a more sedentary lifestyle or other confounding factors |
| 6. Short-term/ Cross-Sectional Studies | Short-term experimental results of many studies do not attempt to capture long-term BMI changes. | Limited number of longitudinal studies presents a problem in assessing the relationship between LHF advertising and childhood obesity |
| 7. Not Accounting for Differences in Ads | Studies often lump all LHF food ads together; effect differs by ad type (e.g., sugary drinks vs. snacks) and ad effectiveness | It is well documented that some ads are more effective than other ads; the assumption that all ad exposures result in equal effectiveness is inappropriate |
| 8. Publication Bias | Findings showing no effect have been shown to be less publishable in academic journals. | Studies claiming societal harm from a practice are more likely to draw attention |
| 9. BMI or other variables self-reporting | Many studies rely on self- or parent-reported outcome measures including BMI | Reporting error is possible for multiple reasons, including embarrassment and social desirability bias |
| 10. Media Platform Issues | It is difficult to track exposure across different platforms such as digital, broadcast, and streaming. etc. | Some studies contain faulty measures of overall media platforms |
| 11. Correlation vs. causation | As with all research, correlation alone does not demonstrate causation. | In observational and experimental studies, confounding factors can play a key role and interfere with the ability to infer a causal relationship between variables. |
Longitudinal studies provide the strongest test of causality, and here the evidence is decisive. The few long-term studies that measure exposure to LHF advertising and track BMI over time find no relationship. Folkvord et al. (2016), for instance, compared children exposed to unhealthy food advergames with those exposed to healthy cues. While the children in the ‘unhealthy group’ did eat more snacks immediately after exposure, there was no association with their BMI two years later. As a result, the authors posited that BMI outcomes are a function of habitual eating patterns and family factors and not advertising.
Similarly, Zimmerman and Bell (2010) analysed data from more than 1,700 children and found no link between commercial television exposure and childhood obesity, once confounding factors such as parental weight, socioeconomic status, and physical activity were controlled for. Ads were not the explanation; lifestyle patterns were.
These findings are not outliers. They are representative of the broader scientific evidence which shows that advertising is at best a weak force influencing short-term choices and behaviour, with no established link to long-term effects on children’s weight gain.
Advertising does not increase category consumption
The conceptual framework linked most closely to the effects of advertising on primary demand is the product life cycle (PLC). The PLC is a foundational concept in marketing theory2, central to planning marketing strategy and product management, and providing precise prescriptions for advertising strategy.
As shown in Figure 1, the PLC charts out sales in a product category over time. Regarding advertising, one of the central tenets of the PLC is that when products reach the mature stage of the life cycle (i.e., the growth rate of category sales slows and then levels off), the role of advertising is to encourage brand switching (e.g., from Pepsi to Coca-Cola) as opposed to increasing overall demand for the product category (e.g., overall demand levels for soda pop).
Earlier in the life cycle, when the product category is not well known (e.g., as with some AI recommender systems or virtual reality devices now), it makes sense to promote primary demand by focusing on the product’s function and general advantages, as overall sales and profits grow rapidly. However, by the maturity stage of the life cycle, sales level off, and the emphasis changes to differentiation and developing and/or maintaining preference for the advertised brand (i.e., the battle of the brands). As a result, advertising at this stage does not increase primary demand for the category.
In the decline stage of the life cycle, the emphasis on advertising shifts to reminder advertising aimed at defending market share and, again, is not focused on building primary demand, as category sales are falling.
Figure 1: The Product Life Cycle (Adapted from Kotler, Keller and Chernev 2022)
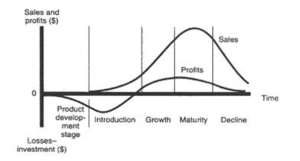
Food categories relevant to LHF policy—crisps, sugary drinks, chocolate, cereals—are all highly mature. In such categories, the role of advertising is not to convince the population to consume more calories overall, but to influence brand preference among consumers who already participate in the category. These conclusions come from decades of econometric research using national advertising spending and consumption data.
The academic literature on the impact of advertising expenditures, culminating in an authoritative study published in the Journal of Marketing Research in 2011, has verified the product life cycle to the extent that it is considered a “settled science”. These studies consistently find that:
- Advertising elasticity declines over the product life cycle.
- There is little or no effect of ad expenditures in mature food product categories on overall demand and consumption levels of those products.
- A large number ofempirical studies from the United Kingdom (and elsewhere) have found no meaningful relationship between advertising and category size in established food markets.
- Advertising for mature food products affects market share and brand switching, but not overall consumption, in mature or late-stage food categories (e.g., branded breakfast cereals, confectionery, bottled beverages, snack foods).
This distinction matters enormously for policy. If advertising does not increase total consumption, then restricting advertising does not reduce it. Instead, it reduces competition among brands and affects visibility, not volume. Policymakers sometimes assume that advertising works like a tap: turn it down and consumption will fall. But the empirical evidence shows that advertising is not the tap that controls the flow.
Thus, the central premise behind LHF advertising restrictions, that ads increase overall consumption and therefore contribute to obesity, misunderstands or perhaps wantonly ignores the fundamental role of advertising in mature product categories.
Do advertising restrictions reduce obesity? The evidence suggests not
If advertising caused childhood obesity, restrictions would reduce it. Yet in practice, jurisdictions that have implemented such restrictions have not seen meaningful declines in obesity rates.
Research on the impact of advertising restrictions and bans specifically on less healthy foods (LHF) is limited. However, evidence from other categories such as alcohol consistently shows that advertising restrictions have little to no effect on overall demand. Multiple studies (e.g., Nelson 2006, 2010; Capella et al. 2008) report that full or partial bans do not significantly reduce sales. These studies do identify impact in that advertising restrictions affect brand-level demand, but not category-level consumption, so as previously noted restricting it for mature product categories rarely reduces total consumption.
A handful of studies have examined the impact of LHF advertising restrictions specifically. Berning (2014) found that voluntary restrictions on soft drink advertising reduced children’s exposure but did not reduce consumption, partly because high‑share brands compensated through pricing or benefited via reduced competition. Dubois et al. (2017), modelling a UK potato crisp advertising ban, predicted a minimal impact on category sales and noted likely substitution toward other unhealthy foods.
The most frequently cited example in the UK concerns the Transport for London (TfL) advertising ban on HFSS products. Some modelling studies claim the restrictions could reduce obesity or improve health outcomes. However, these studies use simulated projections, not real data. They assume that small changes in household purchasing persist, that purchase equals consumption, that food waste is minimal, and that no substitution occurs. Again, these assumptions are not supported by evidence.
When we examine actual obesity figures in London since the TfL restrictions came into effect, no decline is observed. Childhood obesity remains persistently high; in some boroughs it has increased3. Adult overweight and obesity rates likewise show no reduction4. The restrictions may have reduced the visibility of certain ads, but they have not solved the problem they were meant to target.
A 2024 Scottish Government review drew heavily on these studies but ultimately concluded that evidence on the effectiveness of advertising restrictions remains limited, inconsistent, and difficult to evaluate.
Broader reviews, including Guarneiri et al. (2022) and Boyland et al. (2022b), report short-term reductions in advertising exposure and some proximal behaviours (e.g., lower intake in experiments). However, they find no clear evidence that such policies reduce aggregate consumption or obesity over time and rate the certainty of evidence as low or very low.
This is not surprising. Advertising restrictions cannot generate changes in BMI if advertising is not the cause of BMI increases in the first place.
Possible solutions: evidence-based interventions
If advertising is not the driver, what interventions do help reduce childhood obesity?
A review of key literature and meta-analyses of programs that have been the most effective in reducing child obesity strongly suggests that multi-faceted behavioural and lifestyle programs that focus on multiple issues are the most effective (see Ho et al., 2013, and Su et al., 2025). Such measures could include a combination of the following:
- Comprehensive lifestyle and behavioural programmes – school- and family-based lifestyle interventions that combine nutrition education, physical activity, and family engagement show measurable reductions in BMI. Safe outdoor spaces, access to sport, and local health promotion initiatives shift behaviours in ways that accumulate over time. These programmes work because they target the determinants that matter: habits, environments and support systems.
- Parental involvement – interventions that involve parents consistently outperform those that do not. Parents shape routines, food availability, sleep patterns and daily structure, areas where obesity risk is mediated.
- School based interventions have also been found to reduce childhood obesity, mainly when focused on increasing physical activity and providing health education alongside improved school meals.
- Social communication campaigns – the available literature indicates that initiative-taking public education programs can reduce childhood obesity. The research makes clear that this effect is usually limited but can increase when combined with wider interventions, such as school nutrition or community education programs. Designing more effective campaigns based on general consumer behaviour, targeting and segmentation, sending clear, actionable messages, and including feedback loops also increase the chances of success. The effect sizes from studies of communication campaigns advocating healthier eating habits indicate that these programs, especially when combined with other initiatives, hold more promise for long-term reductions in childhood obesity than do restrictions on advertising.
These approaches require investment, coordination, and patience – three things advertising restrictions do not require. But unlike advertising restrictions, they have the capacity to change lives.
The need for evidence-led policy
So, does advertising cause childhood obesity? The evidence clearly indicates that it does not. Advertising influences short-term preferences, not long-term BMI or obesity. It shifts brand share within mature markets but does not increase total consumption. In addition, there is no evidence that advertising restrictions reduce long-term BMI levels or obesity rates.
The central paradox of current obesity strategy is that the factor least associated with childhood obesity is the one that receives the greatest regulatory attention. Meanwhile, the factors most strongly associated with obesity – early-life conditions, socioeconomic environment, physical activity, sleep, dietary patterns – are those most neglected in policy design.
This mismatch is not only ineffective; it is counterproductive. Continued focus on advertising may give the appearance of action while delaying the structural interventions that would address the real causes of obesity. Policymakers risk mistaking visibility for effectiveness by preferring the easy option, rather than the challenging, but ultimately effective, interventions.
If the goal is to reduce childhood obesity, then policy must reflect the evidence. Advertising restrictions may be highly visible, but they are a weak and misdirected tool. The real work lies in early childhood interventions, family support, school programmes, community infrastructure, and addressing the socioeconomic gradients that define children’s lives.
Policymakers face a choice. Continue pursuing symbolic gestures that feel strong but achieve little. Or embrace evidence-led strategies that target the determinants that matter.
The health of the next generation depends on choosing the latter.
About the author:
Charles R. “Ray” Taylor is the John A. Murphy Professor of Marketing at Villanova University and a leading figure in advertising research. A PhD graduate from Michigan State University, he has served as President of the American Academy of Advertising and Editor-in-Chief of the International Journal of Advertising since 2008. He has published over 124 peer-reviewed articles, books, and conference papers, earning numerous best paper awards and global recognition for citation impact. An experienced international educator and speaker, he has taught and lectured worldwide. He is also a Senior Contributor to Forbes.com and frequently featured in major media outlets.
Annex: the full list of publications reviewed in support of this paper
Abernethy, A.M., & Teel, J.E. (1986). Advertising regulation’s effect upon demand for cigarettes. Journal of Advertising, 15 (4), 51-55.
Aleid, A. M., Sabi, N. M., Alharbi, G. S., Alharthi, A. A., Alshuqayfi, S. M., Alnefiae, N. S., … & Al Mutair, A. (2024). The impact of parental involvement in the prevention and management of obesity in children: a systematic review and meta-analysis of randomized controlled trials.Children, 11(6), 739.
Ambler, T., & Eagle, B. (2002). The influence of advertising on the demand for chocolate confectionery. International Journal of Advertising, 21(4), 437–454.
Andrews, R.L. & Franke, G. (1996). Dynamics of aggregate response sensitivities to marketing mix variables. Journal of Business Research, 36(2), 145–155.
Arrona-Cardoza, P., Labonté, K., Cisneros-Franco, J. M., & Nielsen, D. E. (2022).The effects of food advertisements on food intake and neural activity: A systematic review and meta-analysis of recent experimental studies. Advances in Nutrition, 14(2), 339–351.
Bagwell, K. (2007). The economic analysis of advertising. In M. Armstrong & R. Porter (Eds.), Handbook of Industrial Organization (Vol. 3, pp. 1701–1844). Elsevier.
Bartels, R. (1988). The History of Marketing Thought (4th ed.). Prentice-Hall.
Marketing Science Institute. (2017). Product Management and Portfolio Strategy. MSI Report No. 17-112.
Berning, J. P. (2014). The effect of voluntary restrictions on television advertising on the demand for carbonated soft drinks. Journal of Agribusiness, 32(1), 101–118.
Borden, N. H. (1944). The economic effects of advertising. Journal of Marketing, 9(2), 137–149.
Boyland, E., McGale, L., Maden, M., Hounsome, J., Boland, A., & Jones, A. (2022a). Systematic review of the effect of policies to restrict the marketing of foods and non-alcoholic beverages to which children are exposed. Obesity Reviews, 23(8), e13447.
Boyland, E., McGale, L., Maden, M., Hounsome, J., Boland, A., Angus, K., & Jones, A. (2022b). Association of food and non-alcoholic beverage marketing with children and adolescents’ eating behaviors and health: a systematic review and meta-analysis. JAMA Pediatrics, 176(7), e221037-e221037.
Boyland, E. J., Nolan, S., Kelly, B., Tudur-Smith, C., Jones, A., Halford, J. C., & Robinson, E. (2016). Advertising as a cue to consume: a systematic review and meta-analysis of the effects of acute exposure to unhealthy food and non-alcoholic beverage advertising on intake in children and adults. The American Journal of Clinical Nutrition, 103(2), 519–533.
Boyland, E. J., Muc, M., Coates, A., Ells, L., Halford, J. C. G., Hill, Z., … Jones, A. (2025). Food marketing, eating and health outcomes in children and adults: a systematic review and meta-analysis. British Journal of Nutrition, 133(6), 781–805.
Calfee, J. E., & Scheraga, C. (1994). The influence of advertising on alcohol consumption: A literature review and econometric analysis. Journal of Advertising, 23(3), 17–29.
Capella, M.L., Taylor, C.R., & Webster, C. (2008). Cigarette advertising bans’ effect on consumption: A meta-analysis,” Journal of Advertising, 37(2), 7–18.
Cairns, G., Angus, K., Hastings, G., & Caraher, M. (2013). Systematic reviews of the evidence on the nature, extent and effects of food marketing to children: A retrospective summary. Appetite, 62, 209–215.
Carins, J. E., & Rundle-Thiele, S. R. (2014). Eating for the better: A social marketing review (2000–2012). Public Health Nutrition, 17(7), 1628–1639.
Chandran, A., Burjak, M., Petimar, J., Hamra, G., Melough, M. M., Dunlop, A. L., … & Knapp, E. (2023). Changes in body mass index among school-aged youths following implementation of the Healthy, Hunger-Free Kids Act of 2010.JAMA Pediatrics, 177(4), 401–409.
Coleman, P. C., Hanson, P., Van Rens, T., & Oyebode, O. (2022). A rapid review of the evidence for children’s TV and online advertisement restrictions to fight obesity. Preventive Medicine Reports, 26, 101717.
Curtin, E., Green, R., Brown, K. A., Nájera Espinosa, S., Chandrasekar, A., Hopkins, L., … & Scheelbeek, P. (2025). The effectiveness of mobile app-based interventions in facilitating behaviour change towards healthier and more sustainable diets: a systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity, 22(1), 122.
Data Reportal (2025). Digital 2026: China. Data https://datareportal.com/reports/digital-2026-china
Day, G. S. (1981). The product life cycle: analysis and applications issues. Journal of Marketing, 45(4), 60-67.
Dubois, P., Griffith, R., & O’Connell, M. (2017). The effects of banning advertising in junk food markets. The Review of Economic Studies, 85(1), 396–436.
Duffy, M. (1999). The influence of advertising on the demand for food. International Journal of
Advertising, 18(4), 409–428.
Franke, G.R. (1994). U.S. cigarette demand, 1961-1990: Econometric issues, evidence, and implications. Journal of Business Research, 30(1), 33-41.
Folkvord, F., Anschütz, D. J., & Buijzen, M. (2016). The association between BMI development among young children and (un) healthy food choices in response to food advertisements: a longitudinal study. International Journal of Behavioral Nutrition and Physical Activity, 13(1), 16.
Giesbrecht, N., Reisdorfer, E., & Shield, K. (2024). The impacts of alcohol marketing and advertising, and the alcohol industry’s views on marketing regulations: Systematic reviews of systematic reviews. Drug and Alcohol Review, 43(6), 1402-1425.
Goel, R. & Morey, M.J. (1995). The interdependence of cigarette and liquor demand. Southern Economic Journal, 62, 451–459.
González Geuder, Á.-J., & Martín-María, N. (2025). Effects of food advertising on youth’s eating behavior: A systematic review of longitudinal studies. Clinical and Health, 36(2), 97-108.
Guarnieri, Leila, Lucas Perelli, Marcos Clausen, Germán Guaresti, Natalia Espinola, Andrea Graciano, and Andrea Alcaraz.Impact of policies restricting advertising, promotion, and sponsorship of sugar-sweetened beverages: A systematic review. Revista Peruana de Medicina Experimental y Salud Pública. 42 (2025): 28-36.
Gurnani, M., Birken, C., & Hamilton, J. (2015). Childhood obesity: causes, consequences, and management. Pediatric Clinics, 62(4), 821-840.
Greater London Authority. (2025). Snapshot of health inequalities in London 2024. Retrieved from https://data.london.gov.uk/download/snapshot-of-health-inequalities-in-london/ff31c2f6-f6ca-4219-ab6c-ffad3c875ae3/ Snapshot%20of%20Health%20Inequalities% 20in%20 London%202024.pdf
Halford, J. C. G., Boyland, E. J., Hughes, G. M., Oliveira, L. P., & Dovey, T. M. (2007). Beyond brand effect: The influence of television food advertisements on food choice in children and adults. Appetite, 49(1), 263–267.
Hamilton, J.L. (1977). The effect of cigarette advertising bans on cigarette consumption, Proceedings of the 3rd World Conference on Smoking and Health, The U.S. Department of Health, Education, and Welfare, 829-840.
Hartnett, N., Gelzinis, A., Beal, V., Kennedy, R., and Sharp, B. (2021). When Brands Go Dark: Examining Sales Trends when Brands Stop Broad-Reach Advertising for Long Periods. Journal of Advertising Research, 61(3), 247-259.
Henry, G. T. (1984). Advertising and aggregate demand: The case of the food and drink industries. International Journal of Advertising, 3(1), 1–16.
Henry, G. T. (1996). Advertising, market growth, and the food sector. International Journal of Advertising, 15(3), 193–208.
Ho, M., Garnett, S. P., Baur, L., Burrows, T., Stewart, L., Neve, M., & Collins, C. (2012). Effectiveness of lifestyle interventions in child obesity: systematic review with meta-analysis. Pediatrics, 130(6), e1647-e1671.
Hodgson, V., Mizerski, D., and Mizerski, K. (2000). The effect of cigarette advertising through its product life cycle. Proceedings of Australian & New Zealand Marketing Academy Conference (ANZMAC), 525-529.
Iveson, A., Hultman, M., & Davvetas, V. (2022). The product life cycle revisited: An integrative review and research agenda. European Journal of Marketing, 56(2), 467–499.
Jacob, C. M., Hardy-Johnson, P. L., Inskip, H. M., Morris, T., Parsons, C. M., Barrett, M., …& Baird, J. (2021). A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. International Journal of Behavioral Nutrition and Physical Activity, 18(1), 1.
Janicke, D. M., Steele, R. G., Gayes, L. A., Lim, C. S., Clifford, L. M., Schneider, E. M., … & Westen, S. (2014). Systematic review and meta-analysis of comprehensive behavioral family lifestyle interventions addressing pediatric obesity. Journal of Pediatric Psychology, 39(8), 809-1
Jernigan, D., Noel, J., Landon, J., Thornton, N., & Lobstein, T. (2017). Alcohol marketing and youth alcohol consumption: A systematic review of longitudinal studies published since 2008. Addiction, 112(Suppl. 1), 7–20.
Jiang, Y., Hu, J., Chen, F., Liu, B., Wei, M., Xia, W., … & Zhang, J. (2025). Comprehensive systematic review and meta-analysis of risk factors for childhood obesity in China and future intervention strategies. The Lancet Regional Health–Western Pacific, 58,1-16.
Khan, R., Suggs, L. S., Tanweer, A., & Bányai, G. (2024). Food advertisement and marketing policies aimed at reducing childhood obesity: A review of existing regulations in high-income countries. Public Health Reviews, 45, 1607103.
Kotler, P., Keller, K. L., & Chernev, A. (2022). Marketing Management (16th ed.). Pearson Education. https://www.pearson.com/us/higher-education/program/Kotler-Marketing- Management-Global-Edition-16e/PGM333524.html.
Lamb, C. W., Hair, J. F., & McDaniel, C. (2024). Principles of Marketing (14th ed.). Cengage Learning.
Lancaster, K.M., & Lancaster, A.R. (2003). The economics of tobacco Advertising: spending, demand, and the effects of bans. International Journal of Advertising, 22(1), 41-65.
Liu, Z., Xu, H. M., Wen, L. M., Peng, Y. Z., Lin, L. Z., Zhou, S., … & Wang, H. J. (2019). A systematic review and meta-analysis of the overall effects of school-based obesity prevention interventions and effect differences by intervention components. International Journal of Behavioral Nutrition and Physical Activity, 16(1), 95.
Mahumud, R. A., Uprety, S., Wali, N., Renzaho, A. M., & Chitekwe, S. (2022). The effectiveness of interventions on nutrition social behaviour change communication in improving child nutritional status within the first 1000 days: Evidence from a systematic review and meta‐analysis. Maternal & Child Nutrition, 18(1), e13286.
McAuliffe, R. (1988). The FTC and the effectiveness of cigarette advertising regulations. Journal of Public Policy & Marketing, 7(1), 49–64
Mintz, O., Steenkamp, J.-B. E. M., de Jong, M. G., & Currim, I. S. (2017). Drivers of metric use in marketing mix decisions: An investigation across the G7, BRIC, and MIST countries (MSI Working Paper Series No. 17-113). Marketing Science Institute.
Nelson, J. P. (1999). Broadcast advertising and U.S. demand for alcoholic beverages. Journal of Advertising, 28(3), 57–68.
Nelson, J. P. (2006). Cigarette advertising regulation: A meta-analysis,” International Review of Law and Economics, 26(2), 195–226.
Nelson, J. P. (2010). Alcohol advertising bans, consumption and control policies in seventeen OECD countries, 1975–2000. Journal of Economic Surveys, 24(2), 313–337.
Nelson, J. P., & Moran, J. R. (2005). Advertising and U.S. alcoholic beverage demand: Systematic review of econometric evidence. International Journal of Advertising, 24(4), 511–541.
NHS (2024a) National Health Survey, Part 1. https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2022-part-1 (published 24 September 2024).
NHS (2024b) National Health Survey, Part 2. https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2022-part-2 (published September 24, 2024).
Norman, J., Kelly, B., Boyland, E., & McMahon, A. T. (2016). The impact of marketing and advertising on food behaviours: evaluating the evidence for a causal relationship. Current Nutrition Reports, 5(3), 139-149.
Office for Health Improvement and Disparities. (2024).Obesity profile: statistical commentary, November 2024 update. Gov.UK. https://www.gov.uk/government/statistics/obesity-profile-november-2024-update/obesity-profile-statistical-commentary-november-2024
Office for Health Improvement and Disparities. (2025). Obesity profile: short statistical commentary, May 2025 update. Gov.UK. https://www.gov.uk/government/statistics/ obesity-profile-may-2025-update/obesity-profile-short-statistical-commentary-may-2025
Ponce-Blandón, J. A., Pabón-Carrasco, M., Romero-Castillo, R., Romero-Martín, M., Jiménez-
Picón, N., & Lomas-Campos, M. M. (2020). Effects of advertising on food consumption preferences in children. Nutrients, 12(11), 3337.
Poorolajal, J., Sahraei, F., Mohamdadi, Y., Doosti-Irani, A., & Moradi, L. (2020). Behavioral factors influencing childhood obesity: a systematic review and meta-analysis. Obesity Research & Clinical Practice, 14(2), 109-118.
Rozendaal, E., & Buijzen, M. (2023). Children’s vulnerability to advertising: an overview of four decades of research (1980s–2020s).International Journal of Advertising, 42(1), 78–86.
Russell, S. J., Croker, H., & Viner, R. M. (2019). The effect of screen advertising on children’s dietary intake: A systematic review and meta-analysis. Obesity Reviews, 20(4), 554–568. https://doi.org/10.1111/obr.12812
Sahoo, K., Sahoo, B., Choudhury, A. K., Sofi, N. Y., Kumar, R., & Bhadoria, A. S. (2015). Childhood obesity: causes and consequences. Journal of Family Medicine and Primary Care, 4(2), 187-192.
Salinsky, Eileen. “Effects of food marketing to kids: I’m lovin’it?” (2006). Report to the Institute of Medicine. (Issue Brief 814). https://www.ncbi.nlm.nih.gov/books/NBK560001/
Scottish Government. (2024). Restrictions on out of home advertising of food and drink high in fat, sugar and salt: Rapid evidence review. Government of Scotland. https://www.gov.scot/publications/restrictions-out-home-advertising-food-drink-high-fat-sugar-salt-rapid-review-evidence-united-kingdom/
Sethuraman, R., Tellis, G. J., & Briesch, R. A. (2011). How well does advertising work? Generalizations from meta-analysis of brand advertising elasticities. Journal of Marketing Research, 48(3), 457–471.
Simmonds, M., Llewellyn, A., Owen, C. G., & Woolacott, N. (2016). Predicting adult obesity from childhood obesity: a systematic review and meta‐analysis. Obesity Reviews, 17(2), 95-107.
Smith, J. D., Fu, E., & Kobayashi, M. A. (2020). Prevention and management of childhood obesity and its psychological and health comorbidities. Annual Review of Clinical Psychology,16(1), 351-378.
Stautz, K., Brown, K. G., King, S. E., Shemilt, I., & Marteau, T. M. (2016). Immediate effects of alcohol marketing communications and media portrayals on consumption and cognition: A systematic review and meta-analysis. BMC Public Health, 16, Article 465.
Stuart B., & Panico L. (2016). Early-childhood BMI trajectories: evidence from a prospective, nationally representative British cohort study. Nutrition and Diabetes, 6(3), e198-e198.
Sturgess, W. (1982). Advertising expenditure and aggregate consumption: A time-series analysis, 1969–1980. International Journal of Advertising, 1(4), 263–276.
Su, X., Hassan, M. A., Kim, H., & Gao, Z. (2025). Comparative effectiveness of lifestyle interventions on children’s body composition management: A systematic review and network meta-analysis. Journal of Sport and Health Science, 14, 101008.
Thomas, C., Breeze, P., Cummins, S., Cornelsen, L., Yau, A., & Brennan, A. (2022). The health, cost and equity impacts of restrictions on the advertisement of high fat, salt and sugar products across the transport for London network: a health economic modelling study. International Journal of Behavioral Nutrition and Physical Activity, 19(1), 93.
Torbahn, G., Jones, A., Griffiths, A., Matu, J., Metzendorf, M. I., Ells, L. J., … & Brown, T. (2024). Pharmacological interventions for the management of children and adolescents living with obesity—An update of a Cochrane systematic review with meta‐analyses. Pediatric Obesity,19(5), e13113.
Trust for London. (2026). Childhood obesity for children in Year 6 by London borough (2014/15 and 2024/25). Trust for London. Retrieved January 2026, from https://trustforlondon.org.uk/data/child-obesity/
Wang, Y., Cai, L., Wu, Y., Wilson, R. F., Weston, C., Fawole, O., … & Segal, J. (2015). What childhood obesity prevention programmes work? A systematic review and meta‐analysis. Obesity Reviews, 16(7), 547-565.
Weng, S. F., Redsell, S. A., Swift, J. A., Yang, M., & Glazebrook, C. P. (2012). Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Archives of disease in childhood, 97(12), 1019-1026.
Yau, K. W., Tang, T. S., Görges, M., Pinkney, S., Kim, A. D., Kalia, A., & Amed, S. (2022). Effectiveness of mobile apps in promoting healthy behavior changes and preventing obesity in children: systematic review. JMIR Pediatrics and Parenting, 5(1), e34967.
Zarnowiecki, D., Mauch, C. E., Middleton, G., Matwiejczyk, L., Watson, W. L., Dibbs, J., … &
Golley, R. K. (2020). A systematic evaluation of digital nutrition promotion websites and apps for supporting parents to influence children’s nutrition. International Journal of Behavioral Nutrition and Physical Activity, 17(1), 17.
Zimmerman, F. J., & Bell, J. F. (2010). Associations of television content type and obesity in children. American Journal of Public Health, 100(2), 334–340.